Fall 2021 Newsletter

By Dr. Jennifer Peszka, Professor, Psychology
and Dr. Anne Goldberg, Professor, Sociology/Anthropology
Students: Lauren Allen (Anthropology), Noura Musallam (Psychology), and Chloe Cunningham (Anthropology)
Hendrix College
Prior research has shown the importance of social networks in healthy aging. And yet, one of the hallmarks of the COVID-19 pandemic has been calls for limiting social interactions (lockdowns and social distancing). During Spring 2020, Hendrix College and AGEC conducted a telephone survey to examine social connection and isolation in older Arkansans during the COVID-19 pandemic.
About the participants
8745 Arkansans answered the automated phone call and 867 completed the survey. 41.5% of the participants were between 65 and 74 years old, and 58.5% were 75 years old or older. 83.4% identified as White, non-Hispanic; 9.2% as Black; .3% as Hispanic; and 7.1% as other, preferred not to answer, or mixed. 60.2% identified as women, 35.9% as men, and 3.9% as other or preferred not to answer. To examine economic status, they indicated how often they worry about paying their monthly bills. 7% said always, 17.6% said frequently, 35% said seldom, and 40.4% said they never worry about paying their bills.
What they told us
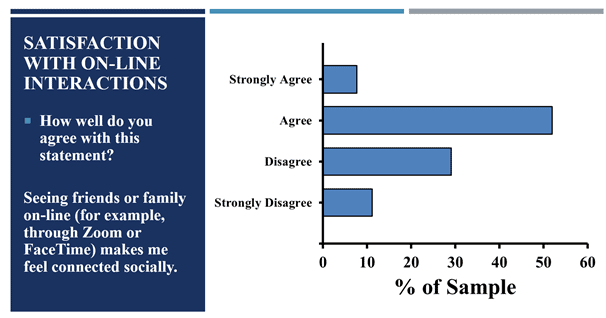
Frequency of interactions: In-person interactions during COVID (the 6 months prior to survey completion) were low, 39.4% of participants reported seeing friends and family living outside of their homes in person twice a month or less. And only 30.8% of them were seeing friends and family in person multiple times a week. These older Arkansans interacted specifically with younger generations of family and friends less frequently during the pandemic than before. 41.1% reported either a lot less frequent or completely stopping social interactions during the pandemic compared to pre-pandemic activities, and only 23.7% reported either the same or even more interactions than before. Despite this reduction in social interactions,many of these participants (88.4%) indicated they had a good deal of social interactions through some form of technology (online, on the telephone, or using some other technology). And that 59.7% of them felt that seeing friends or family on-line (e.g., Zoom or FaceTime) did make them feel connected socially (See Figure 1).
How the pandemic changed social interactions: Before the pandemic, 26.1% reported that they were spending time online or in-person with organized social groups multiple times per week, but during the pandemic this number fell to 14.8%. Before the pandemic, 31% were rarely spending time with organized social groups (less than once a month), but during the pandemic, this rose by 10% to 40.7%.
Satisfaction with social interactions: Before the pandemic, 93% reported they were somewhat or very satisfied with their level of social connection, while that number reduced by a third to 67.2% during the pandemic (See Figure 2). Findings showed that before COVID-19 people were happy, but became less satisfied with their social connection during the pandemic. This decline occurred whether or not participants knew someone who was severely impacted by the virus. People with more technological social interactions, which augmented declining in-person social interactions, had greater satisfaction with their social connectedness compared to people with less technological social interactions. This relationship occurs regardless of the respondent’s level of extraversion. Women were more likely to use technology for social interaction than men during the COVID-19 pandemic, and yet, women were less likely than men to be satisfied by their social interactions during the pandemic. Last, people with the least financial security were using technology to interact socially at a lower rate and were less satisfied with their social interactions during the pandemic than people who had more financial security.
Summary: In person social interactions and satisfaction with social interactions went down during the pandemic. While not a completely satisfying replacement, supplementing lost social interactions with technology did help buffer some of the negative impact on satisfaction for some participants. Therefore, making sure that technology interactions are accessible to all older Arkansans is a worthy goal.